When you take more than one medication, something invisible is happening inside your body. Two drugs might be working against each other, or one might be making the other dangerously strong. These are called drug-drug interactions-and they’re more common than most people realize. In fact, about 1 in 20 hospital admissions among older adults are caused by these hidden clashes between medications. Understanding how they work isn’t just for doctors. If you’re on multiple prescriptions, supplements, or even over-the-counter pills, knowing the basics could keep you out of the emergency room.
What Exactly Is a Drug-Drug Interaction?
A drug-drug interaction (DDI) happens when one medicine changes how another one works. This doesn’t mean the drugs are chemically reacting like in a lab. Instead, it’s about how your body handles them. There are two main ways this happens: through your body’s chemistry (pharmacokinetic) or through how they affect your cells (pharmacodynamic).
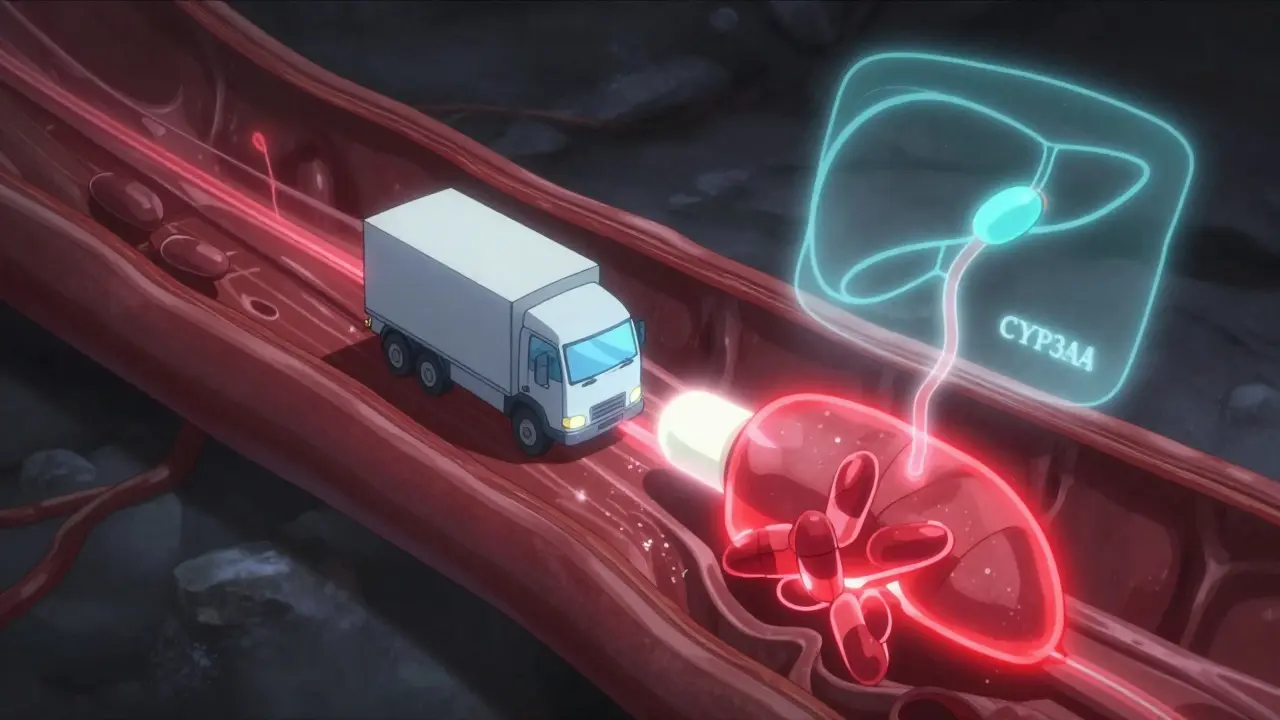
Think of it like traffic. One drug might be a truck slowing down another drug’s path through your bloodstream. Or, two drugs might both be trying to turn on the same switch in your heart, and together they overload it. Both scenarios can be dangerous-even if each drug is perfectly safe on its own.
Pharmacokinetic Interactions: How Your Body Moves the Drugs
This is the most common type of interaction. It’s all about what happens to a drug after you swallow it: how it’s absorbed, distributed, broken down, and cleared out. Four major systems control this process, and drugs can interfere with any of them.
- Absorption: Some drugs change the pH of your stomach or slow down gut movement. For example, antacids can make it harder for ketoconazole (an antifungal) to get into your bloodstream, reducing its effectiveness.
- Distribution: Many drugs bind to proteins in your blood to travel around. If two drugs compete for the same protein, one can get pushed out into the bloodstream, increasing its effect. Warfarin (a blood thinner) and phenylbutazone (an old painkiller) used to cause dangerous bleeding because of this exact mechanism.
- Metabolism: This is where most serious interactions happen. Your liver uses enzymes-especially the CYP450 family-to break down drugs. CYP3A4 alone handles about half of all prescription medications. If one drug blocks this enzyme (like grapefruit juice or ketoconazole), the other drug builds up. Simvastatin, a cholesterol drug, can rise 10 to 20 times higher when taken with ketoconazole. That spike can cause muscle damage so severe it leads to kidney failure.
- Excretion: Your kidneys and liver remove drugs from your body. If a drug blocks the transporters that move others out (like P-glycoprotein), levels can climb. Digoxin, used for heart rhythm, can double in concentration when taken with verapamil, raising the risk of fatal heart rhythms.
These interactions are ranked by severity. A strong inhibitor can raise a drug’s concentration by more than five times. A moderate one might increase it two to five times. Even weak interactions matter if you’re on a drug with a narrow safety window-like lithium or warfarin.
Pharmacodynamic Interactions: When Drugs Talk to the Same Target
This type doesn’t change drug levels. Instead, it changes how the drugs affect your body. Two drugs might team up to overstimulate a system-or cancel each other out.
- Synergistic effects: When two drugs amplify each other. For example, combining fluoroquinolone antibiotics (like ciprofloxacin) with macrolides (like azithromycin) can prolong the QT interval on an ECG. This can trigger torsades de pointes, a life-threatening heart rhythm. Studies show this combo increases the risk by over five times compared to either drug alone.
- Antagonistic effects: One drug blocks the other. Naloxone, used to reverse opioid overdoses, works this way. It kicks opioids off brain receptors, stopping the high-and the breathing slowdown.
- Opposing effects: One drug raises blood pressure, another lowers it. But sometimes, they don’t cancel out cleanly. ACE inhibitors (like lisinopril) and potassium-sparing diuretics (like spironolactone) both increase potassium levels. Together, they can push potassium up by 1.0 to 1.5 mmol/L-enough to stop your heart.
Who’s at Risk? The Real-World Impact
It’s not just elderly patients on a dozen pills. Anyone taking more than three medications is at higher risk. The Beers Criteria, updated in 2019, lists 30 dangerous combinations for older adults. One of the most common? NSAIDs (like ibuprofen) with blood thinners. This combo triples to quintuples your bleeding risk.
Real data from the FDA’s adverse event database shows that between 2010 and 2020, nearly 13,000 reports linked to DDIs involved warfarin, antidepressants, or anticoagulants. Warfarin alone showed up in almost 30% of those reports. That’s not because it’s weak-it’s because it’s precise. Too little, and you risk a clot. Too much, and you bleed internally.
These interactions cost the U.S. healthcare system $1.3 billion a year. Most of that comes from hospital stays due to bleeding from anticoagulant combos or muscle breakdown from statins. And it’s preventable.
Genetics and Personal Risk
Not everyone reacts the same. Your genes determine how fast you break down certain drugs. CYP2D6, for example, is a liver enzyme that turns codeine into morphine. About 1 in 10 people have a version of this gene that makes them ultrarapid metabolizers. They turn codeine into morphine too fast. If they also take a CYP3A4 inhibitor (like fluconazole), the morphine levels spike dangerously. That’s why CPIC guidelines now recommend avoiding codeine entirely in these patients.
On the flip side, poor metabolizers (about 7% of Caucasians) can’t break down drugs like tamoxifen or antidepressants well. Their levels stay too high, causing side effects even at normal doses. This isn’t rare. It’s common-and it changes how interactions play out.
What’s Being Done? Alerts, Apps, and AI
Hospitals and pharmacies use computer systems to warn about DDIs. But here’s the problem: 80 to 90% of those alerts are false. Doctors get so many warnings they start ignoring them. One study found clinicians override 96% of alerts.
That’s changing. New systems like Epic’s “Suggestive Warnings” don’t just flag every combo. They look at context: age, kidney function, other meds, and even lab results. In one trial, this cut high-severity DDIs by 22%.
Specialized tools are helping too. The Liverpool HIV-Drug Interactions Checker updates daily and handles over 350 antiretroviral combos. Pharmacists using these tools reduced dangerous DDIs by 37% in one study of over 12,000 patients.
And now, AI is stepping in. A 2021 study trained a machine learning model on 89 million electronic health records. It predicted DDIs with 94.8% accuracy-far better than old rule-based systems. It’s not perfect, but it’s getting closer to catching the ones that matter.
What You Can Do
You don’t need to be a scientist to protect yourself. Here’s what works:
- Keep a full list of everything you take: Include prescriptions, OTC meds, vitamins, herbs, and supplements. St. John’s Wort, for example, is a powerful CYP3A4 inducer-it can drop cyclosporine levels by 60%, leading to organ rejection in transplant patients.
- Ask your pharmacist: They’re trained to spot interactions. A 2021 study showed pharmacist reviews cut serious DDIs by 37%.
- Know your high-risk meds: Warfarin, digoxin, statins, lithium, and some antidepressants are common culprits. If you’re on one, ask: “Could anything I take make this too strong or too weak?”
- Don’t ignore food interactions: Grapefruit juice? It’s not just for breakfast. It blocks CYP3A4 and can make your statin toxic. Vitamin K-rich foods (kale, spinach) can make warfarin less effective.
- Get genetic testing if you’re on long-term meds: If you’ve had side effects or poor response, ask about CYP2D6, CYP2C19, or CYP3A5 testing. It’s becoming more accessible.
The Bottom Line
Drug-drug interactions aren’t theoretical. They’re happening right now in millions of homes. They’re not always obvious. They don’t always cause symptoms right away. But when they do, the consequences can be deadly.
The good news? Most are preventable. You don’t need to memorize every enzyme or transporter. You just need to know your own meds, ask questions, and trust your pharmacist. The science behind these interactions is complex-but your safety doesn’t have to be.
Can over-the-counter drugs cause dangerous interactions?
Yes, absolutely. Common OTC drugs like ibuprofen, antacids, cold medicines (especially those with pseudoephedrine), and herbal supplements like St. John’s Wort or garlic extract can interact with prescription medications. For example, ibuprofen with warfarin increases bleeding risk, and St. John’s Wort can make birth control, antidepressants, or transplant drugs ineffective. Always check with a pharmacist before combining OTC and prescription meds.
How long do drug interactions last?
It depends on the drugs involved. Some interactions happen immediately, like when two drugs compete for the same protein. Others take days or weeks. For example, if a drug induces CYP3A4 (like rifampin), it can take up to two weeks for enzyme levels to return to normal after stopping it. Inhibitors like ketoconazole may only last as long as the drug is in your system-usually a few days. But if the interaction caused organ damage (like muscle breakdown from statins), recovery can take weeks or longer.
Are herbal supplements safe to take with prescription drugs?
No, not necessarily. Many people assume herbs are natural, so they’re safe. But St. John’s Wort is a potent inducer of CYP3A4 and P-glycoprotein. It can reduce blood levels of cyclosporine, birth control pills, and some antidepressants by over 50%. Garlic and ginkgo can thin the blood and increase bleeding risk with warfarin or aspirin. Always disclose herbal use to your doctor or pharmacist-it’s just as important as listing your prescriptions.
Why do some people get interactions and others don’t?
Genetics, age, liver and kidney function, and even gut bacteria play a role. For example, CYP2D6 poor metabolizers process certain antidepressants and painkillers slowly, so they’re more likely to have side effects-even at normal doses. Older adults often have reduced liver and kidney function, making them more sensitive. And recent research shows gut microbes can break down or activate drugs, changing how they interact. What works for one person might be dangerous for another.
Can I check for drug interactions myself?
You can use online tools like the Liverpool HIV-Drug Interactions Checker or Medscape’s Drug Interaction Checker, but they’re not foolproof. They may miss less common combos, or not account for your full medical history. The best practice is to bring your full medication list to your pharmacist. They have access to clinical databases, can interpret results, and know which interactions are truly risky versus low-priority. Don’t rely on apps alone.
Every year, thousands of people are hospitalized because of drug interactions that could have been avoided. It’s not about fear-it’s about awareness. Know your meds. Talk to your pharmacist. Ask questions. That’s how you stay in control.














